


RERF experts claim their bomb survivor solid cancer mortality data is non-linear

The results of solid cancer mortality analyses in the 0–2 Gy dose range and over the entire follow-up (i.e., 1950–2009) were similar, revealing significant upward curvature in dose response for each sex.[Brenner et al, 2022, page 13]

Figure 1. RERF 2022 update of cancer incidence and mortality.\cite{brenner-2022}[Figure 1]. These are all acute doses, so we can use the Dumbest Graph.
The Infallible Preacher has screwed up again. In The Bomb Survivors and NCRP Commentary 27, I claimed that Grant et al, 2017 was the most recent update of the Radiation Effects Research Foundation (RERF) study of cancer in the bomb survivors.\cite{grant-2017} That was not true.
The most recent update (I now think) is Brenner A, Preston D, Sakata R, Cologne J, Sugiama H, Utada M, Cahoon E, Grant E, Mabushi K, Ozasa K, Comparison of all solid cancer mortality and incidence dose-response in the life span study of atomic bomb survivors, 1958-2009, Radiation Research, May 2022. The reason for listing all the authors, which I rarely do, is to make the point that this an all star line up of the radiation protection establishment. All but one of the authors are associated either with the RERF or the US National Cancer Institute. The exception, Dale Preston, is probably the biggest star of all. Preston has been the personification of the RERF studies for over 40 years. Unlike your highly fallible preacher, these people do speak ex cathedra.
Here are a few quotes from the paper:
Over the entire range of doses, solid cancer mortality dose response exhibited a borderline significant upward curvature among males (P=0.062) and significant upward curvature among females (P=0.010); for solid cancer incidence, as before, we found a significant upward curvature among males (P=0.001) but not among females (P=0.624).\cite{brenner-2022}[page 1]
As reported in (7), there was a significant upward curvature in dose response for all solid cancer incidence among males (P=0.001) but not among females (P=0.624). The all solid cancer mortality dose response exhibited a borderline significant upward curvature among males (P=0.062) with estimated curvature slightly lower than that for cancer incidence. In contrast to solid cancer incidence, the solid cancer mortality dose response exhibited a statistically significant upward curvature among females (P=0.010).\cite{brenner-2022}[p 9]
The solid cancer mortality results for the entire follow-up period (1950–2009) under the current model were similar to those for the 1958–2009 period: significant upward dose response curvature was evident among both males and females (Supplemental Table S1).\cite{brenner-2022}[p 9]
In conclusion, we applied similar analytical methods and rate models to all solid cancer mortality and incidence data in the LSS and found consistent evidence of a modest upward dose response curvature among males for each outcome. By contrast, the upward curvature of comparable magnitude among females was specific to all solid cancer mortality data.
I could bore you with another dozen quotes along the same lines. The paper is surprisingly out front. The new RERF position is their solid cancer mortality data is curved for both sexes. The RERF has already proclaimed the leukemia data to be non-linear.
The cancer incidence data is curved for males; but they cannot reject linearity for females. With respect to the latter, remember the RERF's highly non-standard definition of curved is the ratio of the quadratic to linear coefficient in their fit is at least 0.25. They then do a test to see if the data rejects the linear hypothesis. For the RERF, linearity is the null hypothesis which must be disproved. It's not about finding the best fit. It's whether or not we can defend a linear fit. In 3 of the 4 cases, the answer was no.
Figure 1 shows the updated RERF fits. Two points about this figure.
The High End
As we have seen over and over again in the dose-cancer curves, there is a strong decrease in the slope at the high end.1 In this case, it is particularly obvious for the female incidence data. If you limit your fits to linear and quadratic, this non-linearity perversely favors linear.
The RERF finally acknowledges this high end reduction in slope. The paper calls it the High Dose Effect.
Another difference from the Report 14 model was that we adjusted for “high dose” effect. It was implemented to minimize the influence of individuals with total shielded kerma >4 Gy and considerable uncertainties in dose estimates on dose response parameters. Unlike other modifications to the cancer mortality model, this adjustment substantially enhanced the magnitude of upward curvature in dose response for each sex.
The estimates of sex-specific curvature for solid cancer incidence also increased following adjustment for high dose, although to a lesser extent than those for cancer mortality. The influence of “high dose” survivors on estimation of dose response for all solid cancer is related to the fact that there appears to be a downturn in dose response at very high doses. Whether the downturn is due to unaccounted dose error or cell killing continues to be debated. Collectively, these findings suggest that without allowance for high dose effect our inference about the dose response shape over the full range of doses in the LSS could be biased. However, it is important to recognize that substantial evidence of dose response curvature for all solid cancer is present in the 0–2 Gy range, at doses associated with smaller uncertainties, in mortality data for males and females,
The simplest adjustment was to throw out the highest doses. But the "adjustments" only apply to doses above 4 Gy. Figure 1 shows that the high dose effect extends downward to well below 3 Gy. If the adjustments started at 3 Gy, the female incidence curvature would have increased.
The Low End
For public exposures from nuclear power plant releases, what is counts is the very low end corners of Figure 1, the portion below 0.05 Gy. As usual, the RERF view obscures this all important zone. But that's where most of the RERF data is, and most of that data is below both the Brenner linear and the linear-quadratic fits, Figure 2.
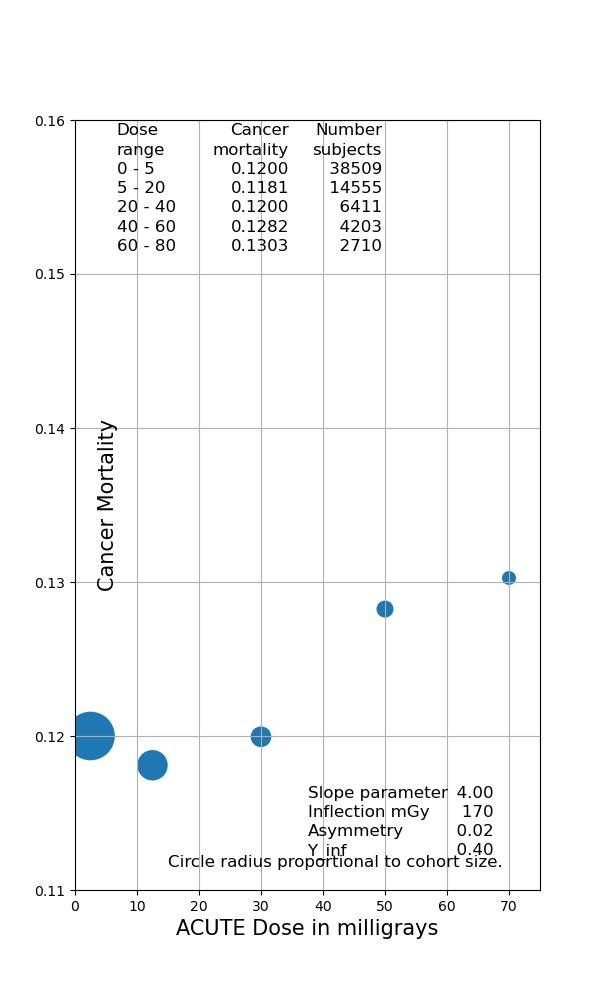
Figure 2. LSS 14 Cancer Mortality below 0.075 Gy.
So we have a high end slope that is smaller than both the linear and linear-quadratic fits and a low end slope that is smaller than both fits. The authors of this paper are all smart people. They know a lot about dose response. You cannot tell me that none of them came up with the obvious solution: an S-shaped fit, especially since sigmoid fits are near standard in dealing with dose response curves. But to my knowledge, the RERF has never publicly tried such a fit.
The RERF has come a long way; but it still has a long way to go. For now though, we must be satisfied with this simple fact. According to the Radiation Effects Research Foundation, their self-proclaimed goldstandard of all radiation dose response data does not support the Linear No Threshold hypothesis.
The GKG suggestion is that the key starting point of cancer is viable misrepairs, mainly from rejoining the wrong ends of two closely spaced Double Strand Breaks in the DNA. Unrepaired cells cannot replicate. One possibility is that if the cell gets hit with two much radiation too fast, the repair process somehow gets disrupted, perhaps due to damage to the repair complexes. Less repairs mean less misrepairs which means less cancers. But this is just a guess. So far the radiation protection community has shown little interest in the High Dose Effect.
It was the U.S. military itself that organized the study of the radiation effects of atomic bombs—a situation akin to granting a criminal credibility in counting their victims.
https://www.pnas.org/doi/full/10.1073/pnas.95.10.5426
When breast cancer incidence after bombing was reported in 1979 (Tokunaga et al, JNCI) in women over 40 at the time of the bombing, there was only 107 breast cancers in a population of 18,464 women over a period of 24 years, which is the main period of occurrence of breast cancer. Today, the lifetime risk of breast cancer is 1 in 8 in the USA.
It is simply impossible to believe results in the fields where the US army is involved.
Let me understand better. "significant upward curvature among males (P=0.001) but not among females (P=0.624)" is comparing the quadratic fit to the 'no-effect' dose-response? Or to the LNT dose-response?
And how can there be such vast differences between male and female?
And the parameters in Figure 2 are those of your SNT fit, not shown?