
The Auto-Genocidal Tragedy of US Nuclear Power, Part 2

This is Part 2 of our serialized presentation of this tragedy in slideshow format. Part 1 is at Auto-Genocidal Tragedy. The full deck is here. We take the story up in 1959. The AEC has just quietly adopted LNT, the harm theory that our bodies cannot repair radiation damage to our DNA. LNT suited the purposes of both those who believed the way to stop WW3 was to stop bomb testing, and those who believed the way to stop WW3 was to emphasize how catastrophic WW3 would be.
The acceptance of LNT put the AEC in an impossible bind. If you combine LNT with a long list of worst case assumptions, a big release of radioactive material could kill tens of thousands of people via cancer. To promote nuclear power, the AEC had to claim that by stringent regulation and meticulous quality assurance programs it could prevent such a release, or at least make it so unlikely that we don’t have to worry about it.
The Negligible Probability Lie is false. Three Mile Island, Chernobyl, and Fukushima made that obvious. You cannot prevent all releases. The probability of the next big release is 1.00. It’s only a question of when. The AEC/NRC was attempting the impossible. There is no limit on the amount of money you can spend attempting the impossible. Or rather the limit is the point where you make nuclear prohibitively expensive. We reached that limit very quickly. By 1980, US plants were costing ten times as much as Oconee, and taking twice as long or more to build.
Which brings us to the Intolerable Harm Lie.
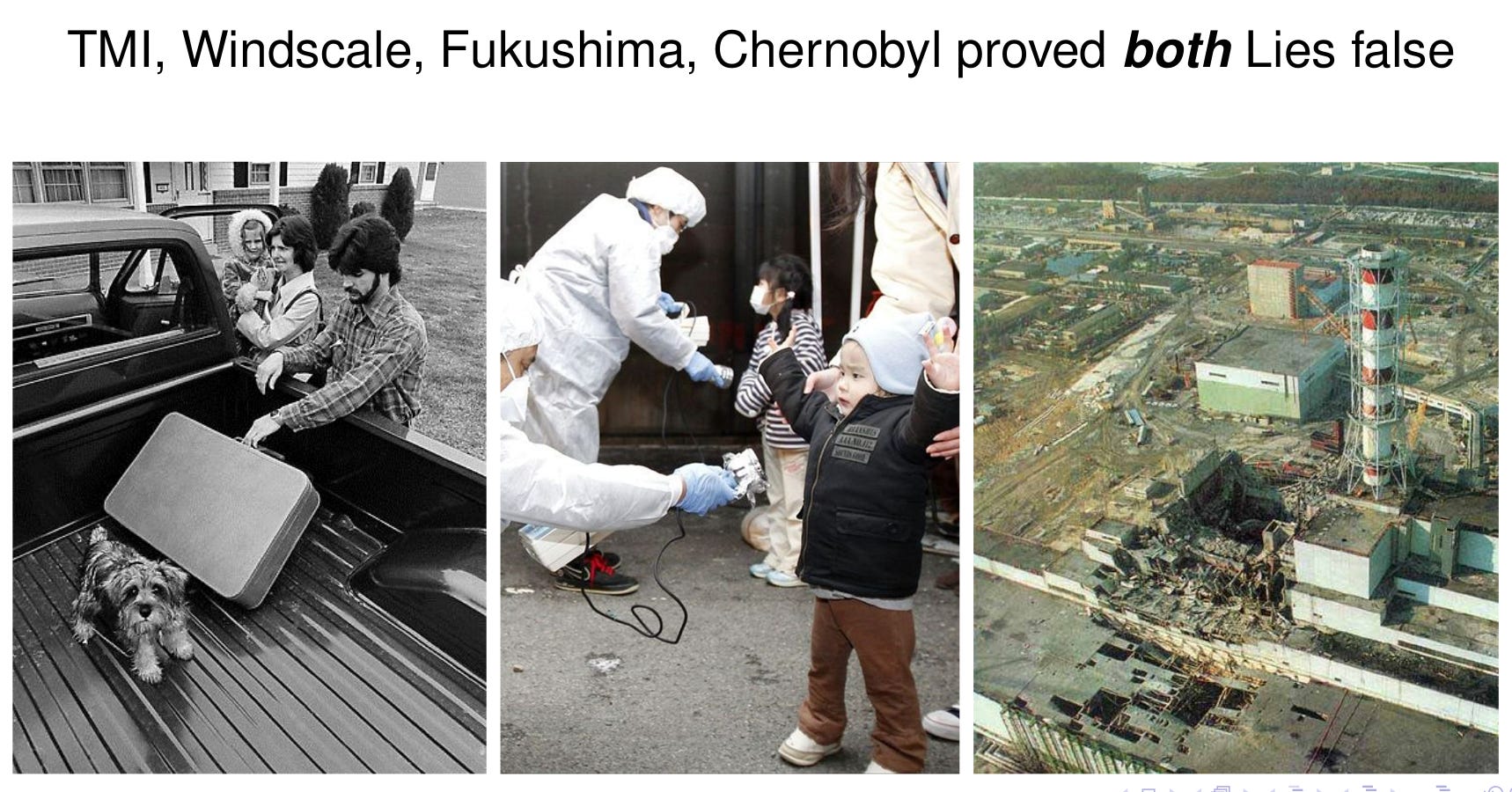
Despite the Negligible Probability claim, we’ve had six big releases from commercial nuclear reactors (three at Fukushima) in about 22,000 reactor years of operation. How has the Intolerable Harm claim held up?
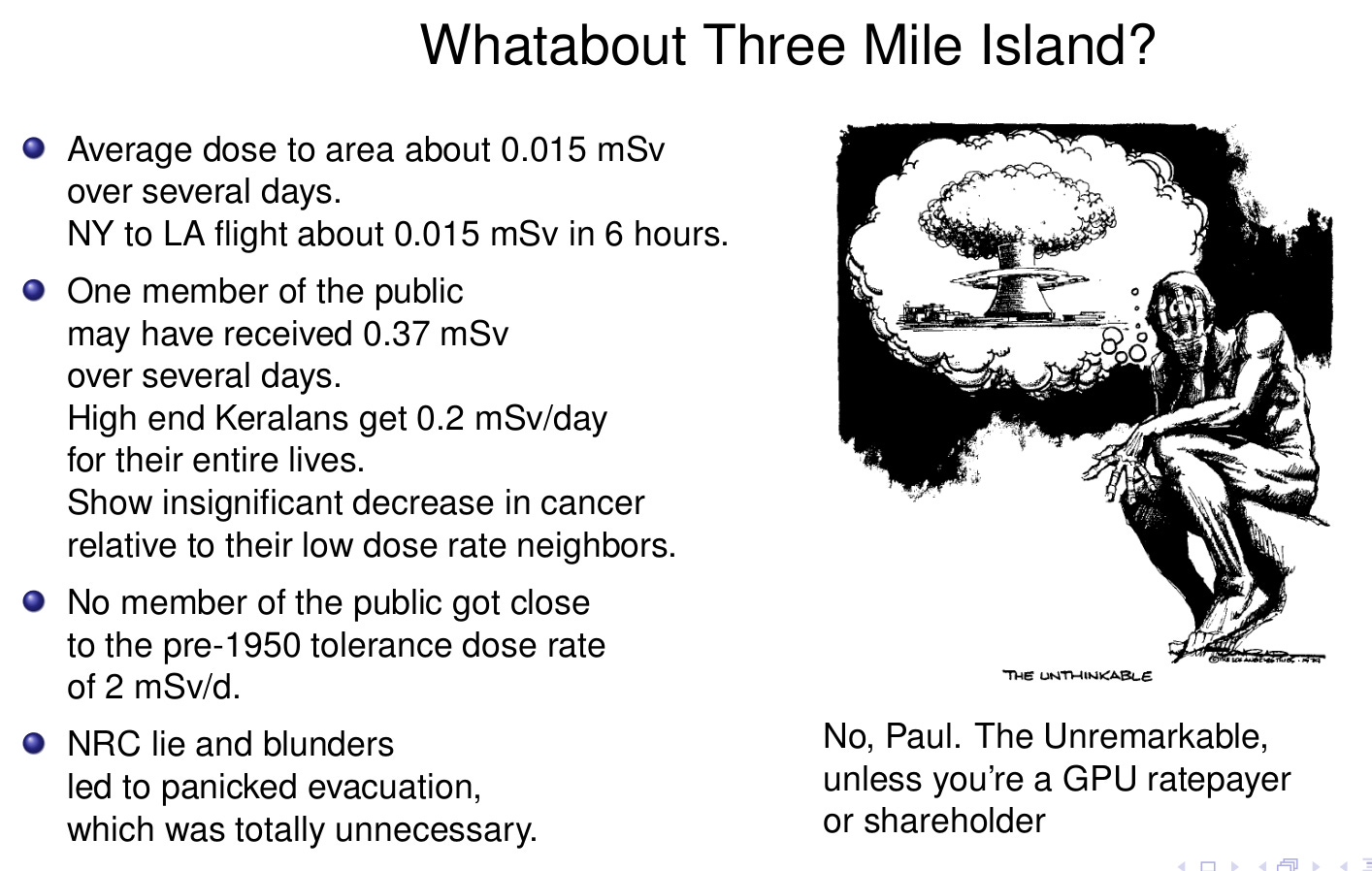
Three Mile Island was a full meltdown of the youngest reactor in the US fleet, the plant subject to the most stringent NRC regulation. The plant was a multi-billion dollar write off; but almost all radioactive material stayed inside containment. NRC preposterously lied to avoid admitting there had been any release; and then concocted an impossible hydrogen explosion in reactor vessel. The area had been pretty calm up to then. Panic ensued. Bishop granted General Absolution. Ten of thousands evacuated. Enormous publicity; famous, effective, and impossible Conrad cartoon showing mushroom cloud emerging from a cooling tower.
From a radiation harm point of view, TMI was a non-event. But TMI exposed the Negligible Probability Lie big time. The public trust in the nuclear establishment was destroyed and with good reason. Few noticed the Intolerable Harm claim was also contradicted.
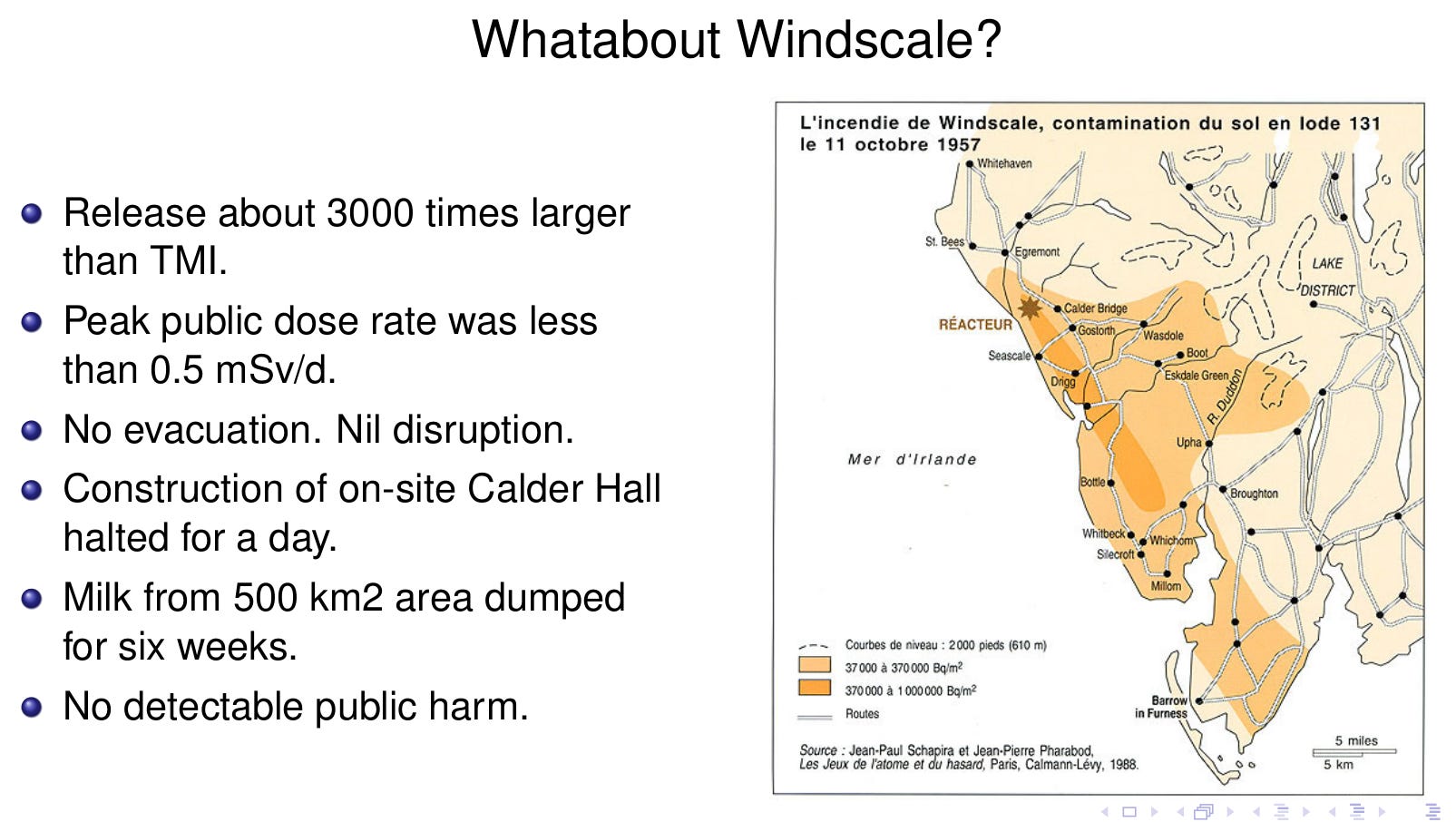
Windscale was a graphite moderated, weapons production reactor in northwest England. In 1957, the graphite caught fire resulting in a large release, 3000 times larger than TMI. The plant had a good relationship with the locals and kept them informed throughout. There was no evacuation, voluntary or involuntary. Construction work at the site was shut down for a day. The only result was destruction of a poorly designed reactor and the loss of some milk. All attempts to reliably detect any increase in cancer in the area have failed.
Windscale not only proved that a big release is not intolerable, it showed that a properly handled release, while extremely expensive for the reactor owner, need not be disruptive for the local community.
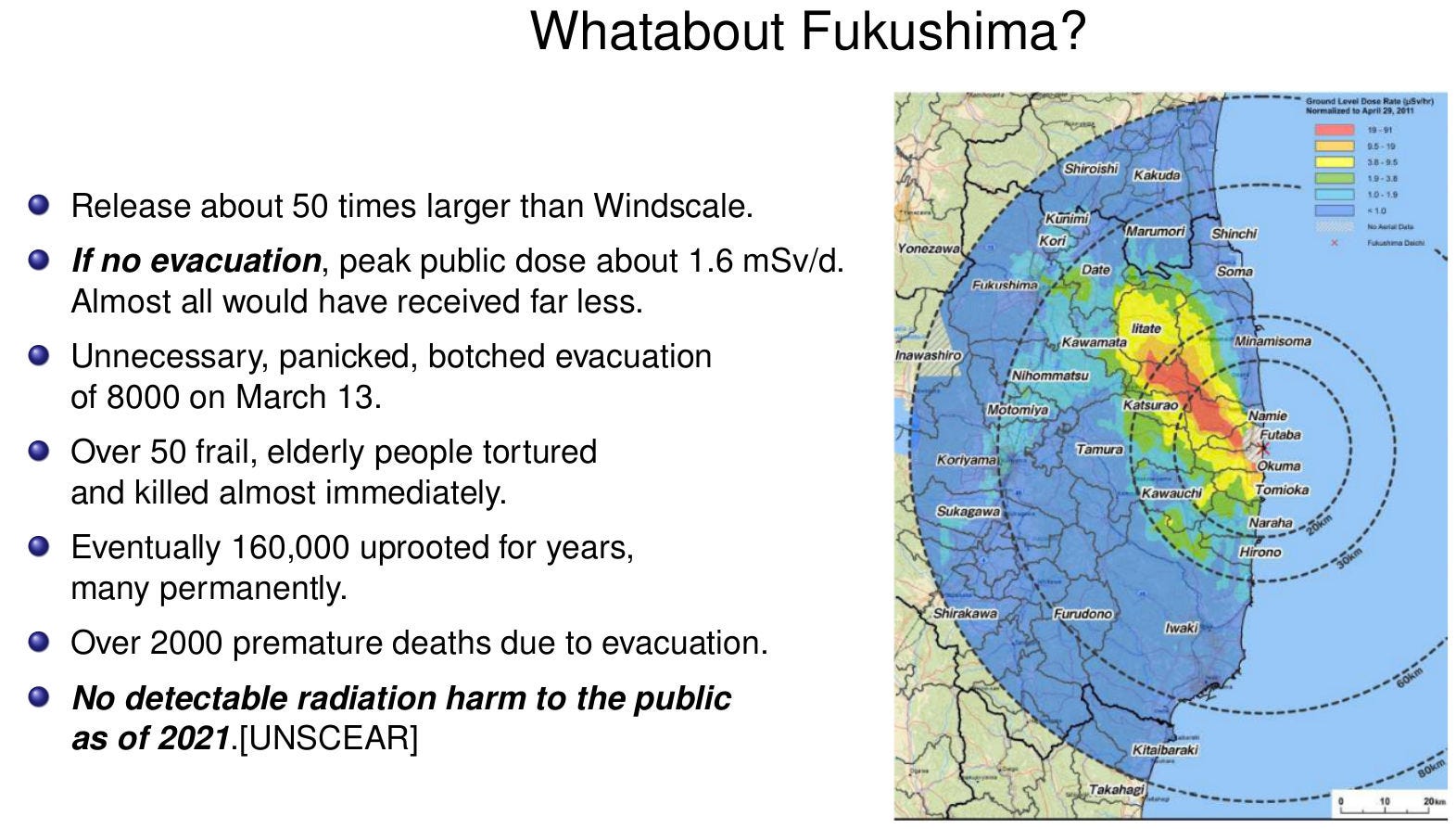
At Fukushima, the peak public dose rate assuming no evacuation would have been less than the pre-1950 ICRP tolerance rate. Ten years later UNSCEAR was unable to detect any increase in cancer in the public, nor does it expect to see any. We can’t even detect any increase in cancer in the plant personnel, many of whom suffered far, far worse dose rate profiles than any member of the public.
The harm was caused by the panicked response. 50 old people murdered almost immediately. 2000+ excess deaths due to unnecessary evacuations and exile. Thousands of premature deaths due to increased coal pollution and increased cost of heating and cooling, from politicians shutting down perfectly good nuclear plants. Auto-genocide miniaturized, but auto-genocide nonetheless.
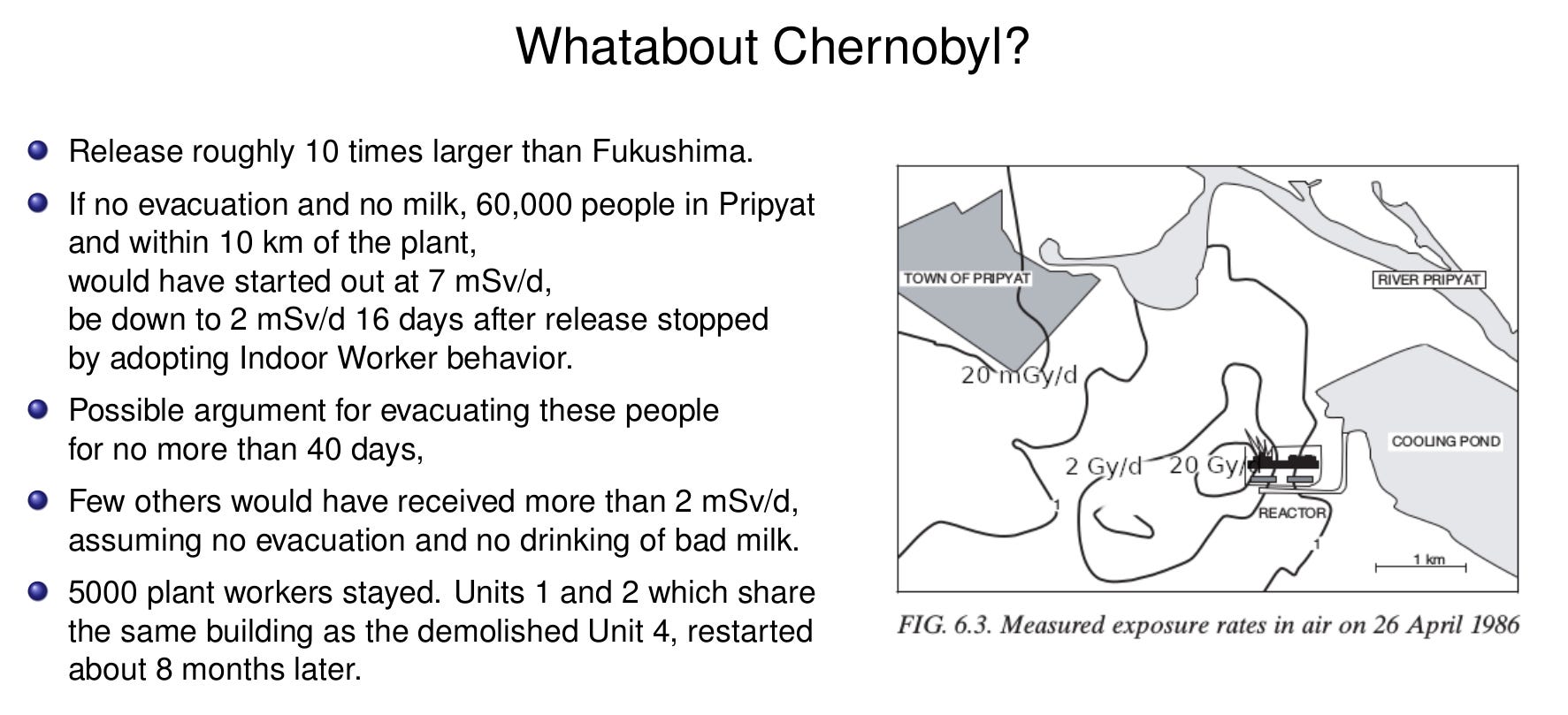
Chernobyl shows the importance of buffer zones. The initial ambient dose rates near the plant are off the chart. 20,000 mGy/d in the Red Forest. Deadly in a few hours. 1,000,000 mGy/d on the Unit 3 roof. Deadly in a few minutes. But the dose rates fall off sharply. The hardest hit parts of Pripyat, 3 km from the plant started off at about 24 mGy/d. As we shall see, this is just below the dose rate, at which we start to see cancer in multi-year exposures. But dose rates in Pripyat were below 2 mSv/d 40 days after the release stopped. This is a factor of ten less than the lowest dose rate at which we have ever detected increased cancer in even multi-decade long exposures. Evacuating Pripyat for more than about 40 days cannot be justified from a radiation exposure point of view.
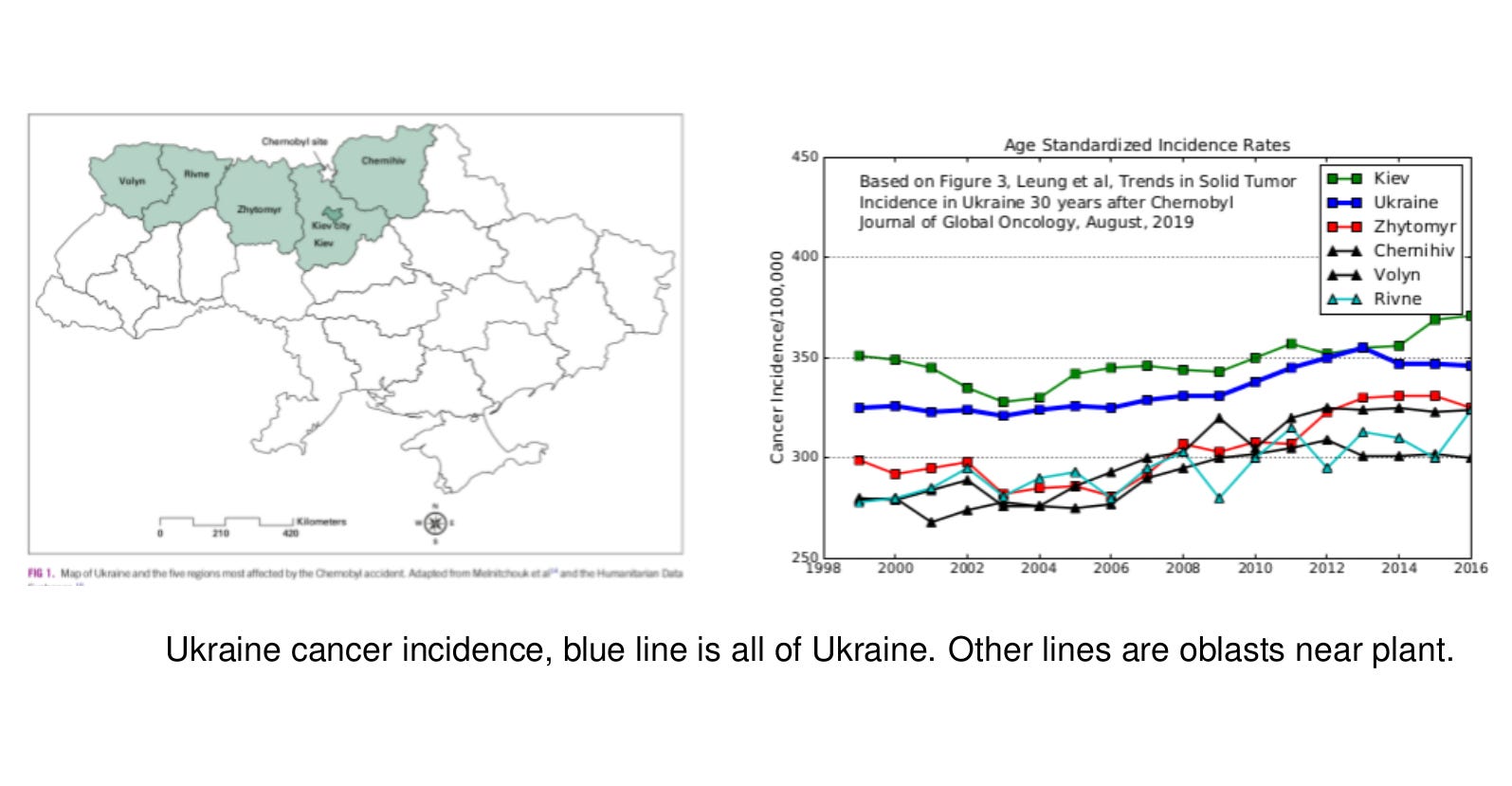
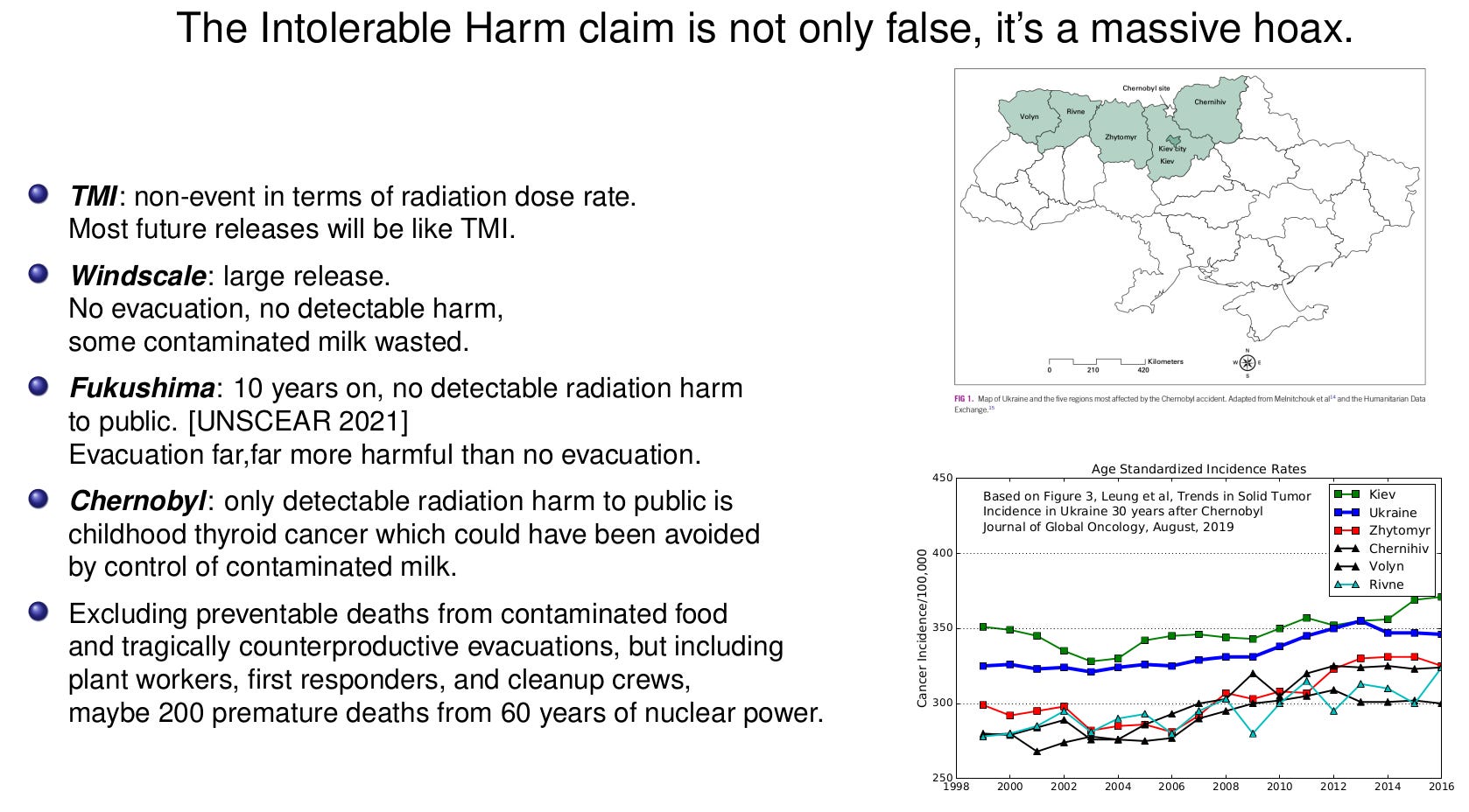
In 2019, 33 years after the release, a team from Harvard Medical School queried the Ukrainian National Cancer Registry.[Leung, 2019] They could find no systematic differences in the solid cancer incidence rates in the districts close to Chernobyl compared to the country as a whole. 33 years on, the 1000’s of cancers predicted at Chernobyl, simply never happened. The Kiev oblast is higher than the Ukraine average, probably because the 3 million person capital has more pollution and better detection. During the release, the plumes were mostly east-west and to the north. Those oblasts had lower cancer rates than the national average, probably because they are highly rural.
According to LNT, there should have been a 3% increase in solid cancers in the surrounding districts.[Cardis, 1996] In a population of 270,000, this should be statistically detectable. The Cardis-1996 reference calculation is the source of the ``official” estimate of an eventual 4000 to 8000 ``deaths” from Chernobyl. Cardis, LNT, and the ``official” number are flat wrong.
In this figure, we can clearly see that the hardest hit areas were to the west of the plant and to the northeast.
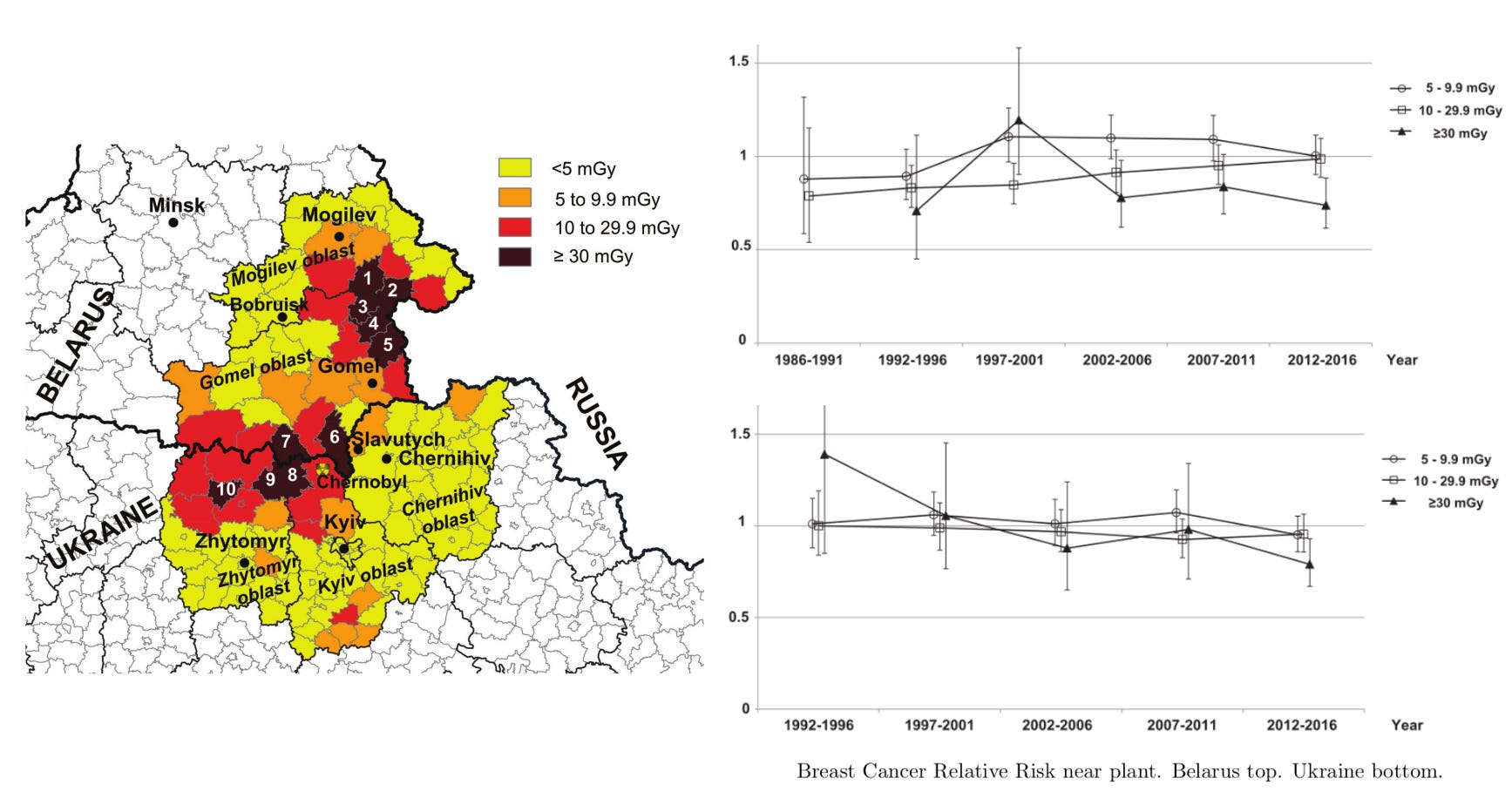
Breast cancer is one of the more radiosensitive diseases. Zupunski et al studied breast cancer incidence in the rayons (roughly counties) close to the plant.[Zupunksi-2021] There was no statistically significant difference in the breast cancer rate between the high dose rayons and the low. If anything, the higher dose rayons tracked below the lower.
Not only have the thousands of deaths failed to materialize; but we have been unable to find even a hint of an increase in cancer in the general public from the Chernobyl release.
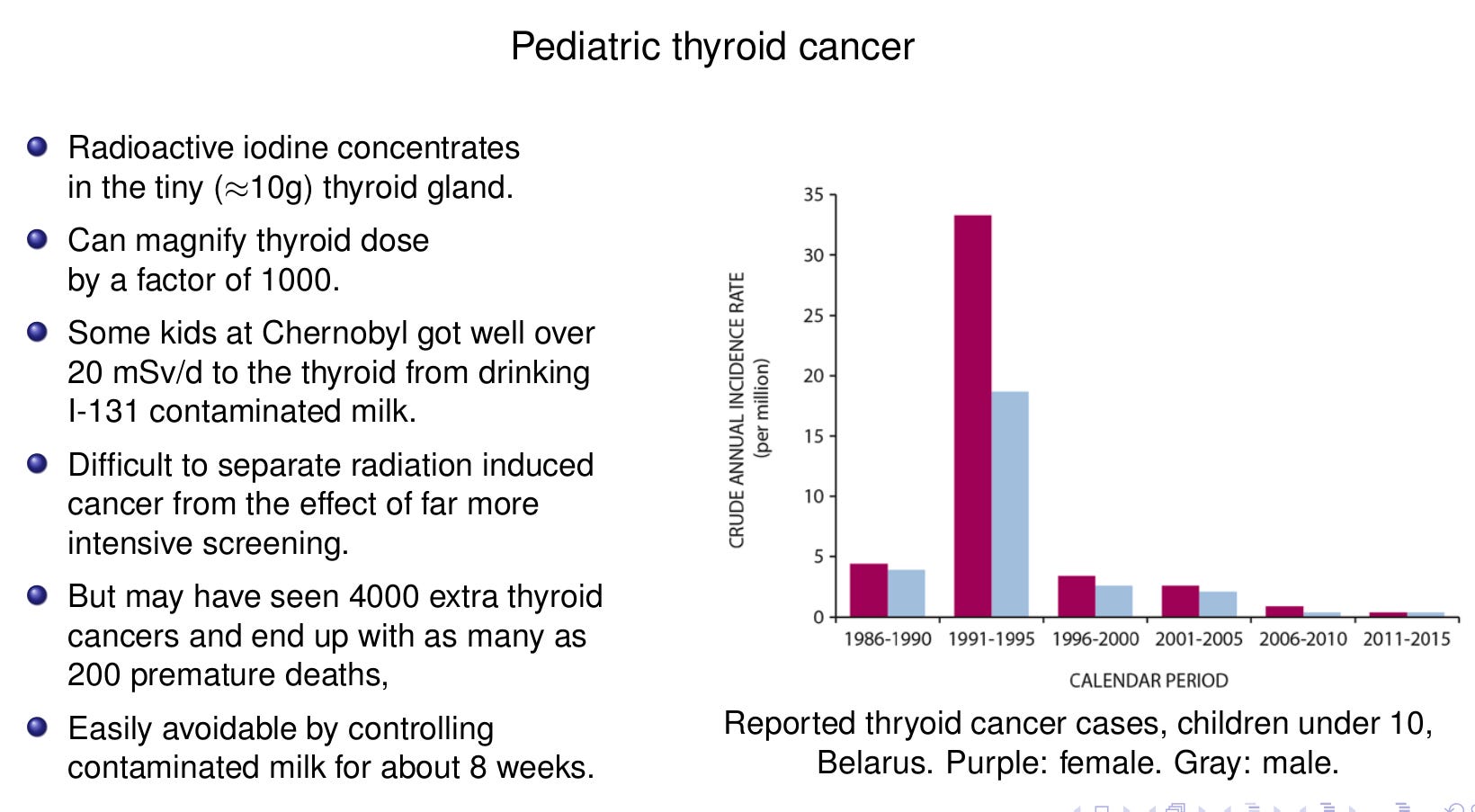
The single exception to no detectable increase in cancer from Chernobyl is childhood thyroid cancer. Radioactive iodine concentrates in the tiny (~10 gram) thyroid gland. This can magnify thyroid dose rates by a factor of 1000. Some kids at Chernobyl got well over 20 mSv/d to the thyroid from drinking I-131 contaminated milk.
The size of the impact is highly controversial. With no special screening, child thyroid cancer detection rates run about 1 in a million. After Fukushima, ~300,000 kids received intensive screening. The resulting detection rate was 640 per million. But there is no evidence this had anything to do with radiation. Thanks to stringent food control, the Fukushima thyroid dose rates were tiny. Control group programs in parts of Japan nowhere near Fukushima came up with similar detection rates.
But the Belarus/Ukrainian kids had still higher incidence and there was a correlation with dose rate. Some of the extra reported cases were undoubtedly radiation related. We could eventually see as many as several hundred premature thyroid cancer deaths from drinking contaminated milk.
The key takeaway is: whatever the number is, it was easily preventable, as Windscale and Fukushima showed. All that’s required is restricting contaminated milk consumption for about 8 weeks, at which point essentially all the radioiodine will have decayed away.
39 years on, the tens of thousands of cancers confidently predicted by LNT at Chernobyl simply never happened. In all four big releases, the only radiation harm to the public, which we have been able to reliably detect, is an increase in childhood thyroid cancer, which could have been prevented by controlling milk for a couple of months.
This raises the obvious and crucially important question: why did we not see those cancers? Why are our bodies so good at handling radiation damage to our DNA?
TO BE CONTINUED
> This raises the obvious and crucially important question: why did we not see those cancers?
There's a very mundane and simple answer to this question: lack of statistical power (and of a control group) to detect very small ERR on the background of 40% lifetime cancer rate.
Let's say my dinner table deflects by 1 mm when I put a 10kg weight in the middle of it. If I put a 10 milligram weight in the middle of it, and I am unable to see it deflecting by 1 nm , does that prove, or even suggest validity of a nonlinear table model? No, it's an ordinary dinner room table in an ordinary room, there's an air conditioning vent right over it.